
PCI in a complex anatomy
Patient description
69 years old male with CCS 3 angina and a previous unsuccessful attempt of PCI to treat RCA chronic total occlusion at a different center was referred to us.
Initial situation
Coronary angiogram revealed a ‘stump’ occlusion of the very proximal RCA; the distal vessel was filled through epicardial collateral vessels from the septal system.

Procedure
Coronary Angiography
Procedure description
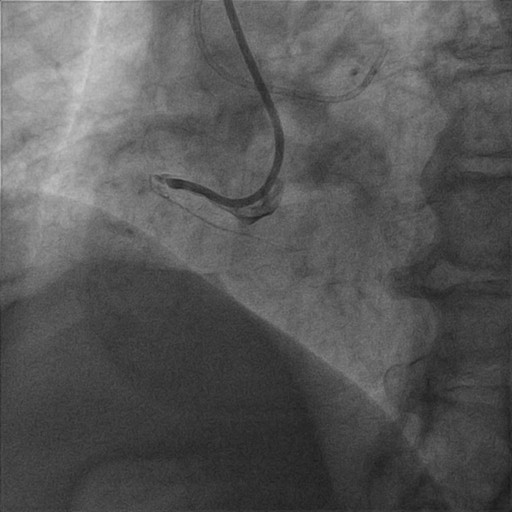
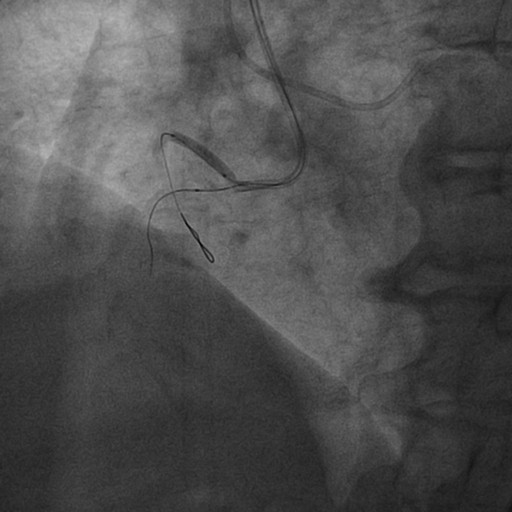
An AL1 guiding catheter through femoral route was used to engage RCA; occlusion crossingwas unsuccesfully attempted by using a Fielder XT wire supportd by a FineCross microcatheter (figure 1).
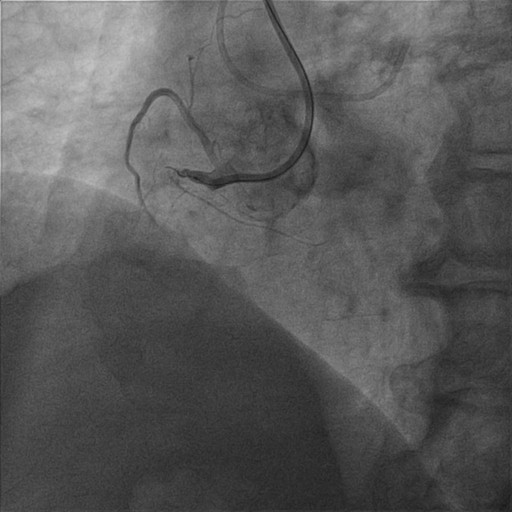
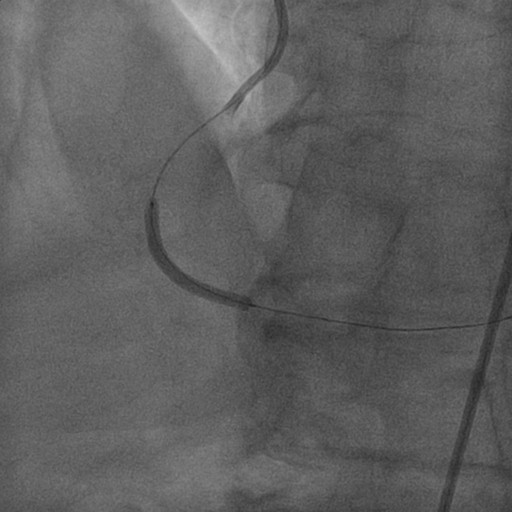
Thus, an anchoring balloon strategy was used by putting a floppy 0.014’’ wire and an inflated 2.0 mm balloon in the conus branch (figure 2).
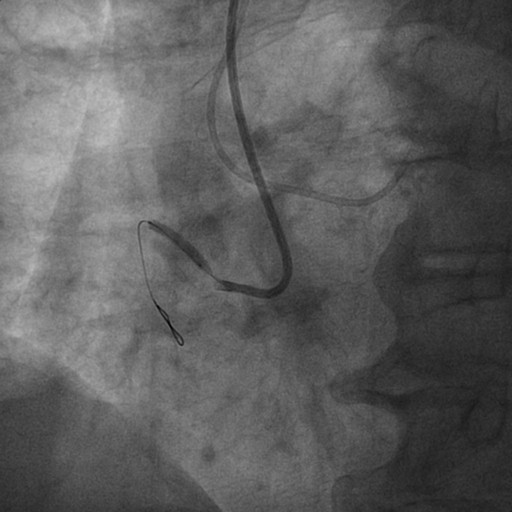
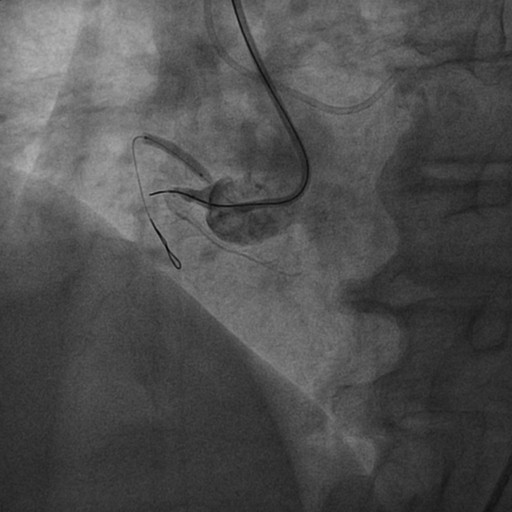
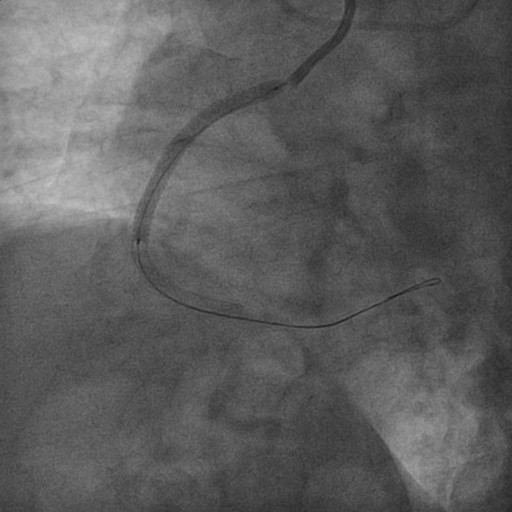
Proximal cap puncture was then performed with a Miracle 12 guidewire (figure 3) then replaced with a hydrophilic wire (figure 4).
After successfully gaining distal lumen, predilation was performed and two dru-eluting stents were successfully deployed from distal to proximal RCA (figure 5).
Final result
Good final result showing the recovery of antegrade flow in RCA and the loss of retrograde filling from the left system.
The patient was safely discharged and he is still asymptomatic at 12-month follow-up.